")
")
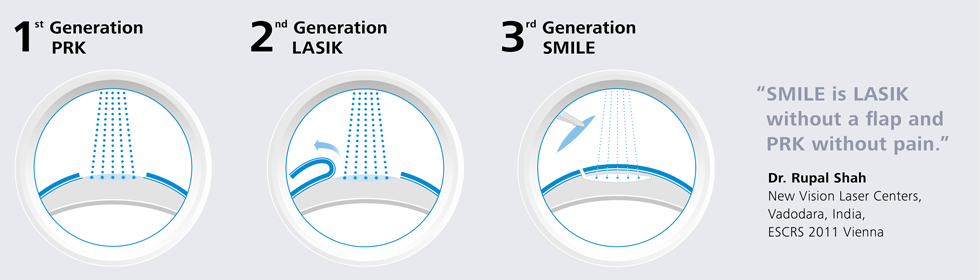
SMILE - the latest frontier in refractive surgery

Since the first operation carried out at the beginning of the 1990s, corneal refractive surgery has undergone an important evolution with improvements in surgical techniques and outcomes as well as shorter recovery times.
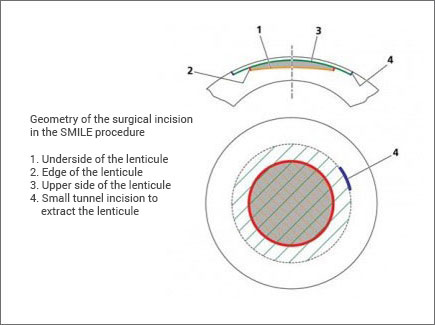
The latest frontier in laser techniques to correct visual disorders is called Small incision lenticule extraction, SMILE, an innovative technique as it is minimally invasive and without the need to create a corneal flap. This surgical procedure uses the latest generation of 500Hz femtosecond lasers (Visumax, Carl Zeiss Meditec) to create a lenticule within the corneal stroma, with a very well-defined geometry in order to correct the refractive error. This lenticule is then extracted through a small incision tunnel in the cornea itself. All this occurs without the use of an excimer laser and without needing to create a corneal flap (as in the LASIK technique). The SMILE procedure produces refractive outcomes similar to those using the LASIK technique, with excellent post-operative results:
- Faster visual and functional recovery times
- Eliminates the risk of complications associated with the creation of a flap
- Increased corneal biomechanical stability
- Lower occurrence of dry-eye in the post-operative phase
The SMILE technique may be used to correct myopia and astigmatism; the use of this technique to correct hyperopia is still under trial so for the moment LASIK or LASEK treatments are still preferred.
FDA clinical trials started in the USA in 2012, and approval of the technique was given by the FDA in September 2016.
Outside of the USA the SMILE procedure is carried out by 150 centres in 38 countries.
Detailed description of the SMILE surgical technique
When the SMILE procedure starts, the operating table is raised so that the patient’s eye is in contact with the suction device which is then activated to keep the eye fixed in the right position while the laser cuts the lenticule and makes the tunnel incision.
First of all the lower interface is created with centripetal force in order to minimise the time that the patient’s central vision remains blurred, and then the upper interface using a centrifugal force. Finally the tunnel incision of 2–3 mm is made, usually superotemporally, which connects the lenticular interface with the corneal surface.
 To prevent any undesired effects on the cornea, such as haziness or opalescence, the two interfaces are created from the endothelium towards the epithelium.
To prevent any undesired effects on the cornea, such as haziness or opalescence, the two interfaces are created from the endothelium towards the epithelium.
The patient is then moved to the surgical microscope for the separation and extraction of the lenticule using micro forceps or a stripper.
When planning the operation the surgeon needs to choose the following parameters:
- Cap thickness
- Cap diameter
- Cap sidecut angle
- Refractive correction
- Lenticule diameter (depending on the optical zone)
- Lenticule sidecut angle
- Minimum lenticule thickness (to make it easier to differentiate the upper from the lower interface)
Dr. Bianchi uses the SMILE technique on suitable patients. Click here for further information.
The SMILE technique has already been adopted by the most experienced surgeons around the world who recognise its surgical and post-operative advantages.